Surgical Design Case Study 4 - Reconstruction and Enhancement
AT: PDR
FOR: NHS
MY ROLE: COMMERCIAL PROJECT MANAGER / DESIGNER

Clinical Background
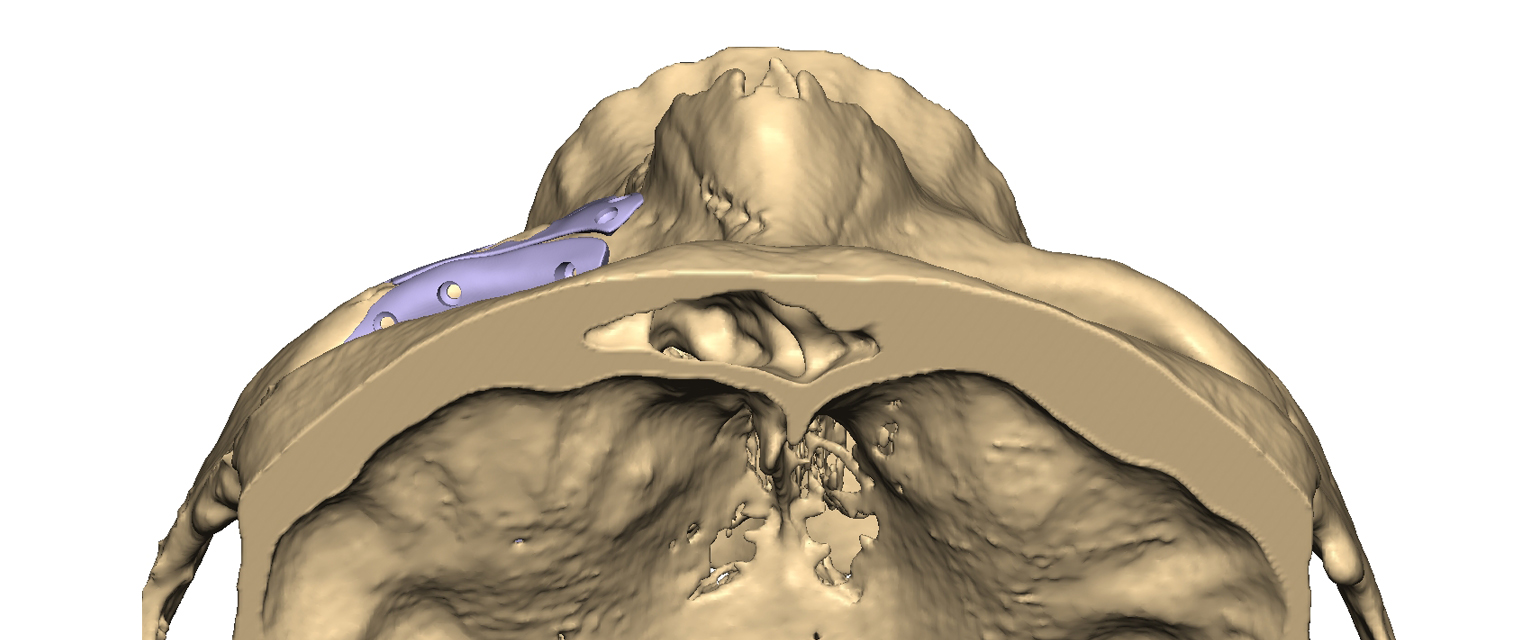
The patient had suffered a traumatic injury some years prior – resulting in the fracturing and displacement of bones in their zygoma, orbit, and maxilla. Initial surgery had resulted in a sub-optimal fixation of the displaced bones – and a mal-positioned eye remained uncorrected. These factors contributed to a significant asymmetry in facial aesthetics. The maxillofacial surgeon approached PDR to assist with designing patient-specific implants to correct the aesthetics of the face and the function of the eye. One piece of metalwork from the initial surgery needed to be removed prior to the new implants being inserted (below, right) and some had to be accommodated by the new implants because it would be left in-situ.

Design
I worked closely with the clinician on this project to plan the surgical procedure digitally, and design patient-specific devices. My carefully structured design process enabled efficient optimisation of the proposed reconstruction whilst ensuring patient safety by anticipating potential problems and constraints. One short online meeting was held to specify the surgical plan, with final device design approval undertaken offline at the surgeon’s convenience.

I segmented the patient’s CT scan-data and created a virtual model as the basis for digital surgical planning. The healthy contralateral anatomy, corresponding to the region of interest, was copied and mirrored. Adjustments were made using smoothing and blending techniques to achieve a best-case fit of the mirrored anatomy against the residual injured bone.
Then, deliberate compromises were determined in collaboration with the surgeon – between the ideal, perfect reconstruction and what would work reliably and safely with the existing metalwork and existing bone. I took advantage of the design freedoms offered by additive manufacture (or 3D printing) to model two implants with varying thicknesses and intricate, organic shapes.
Considerations
The orbital implant was designed to accurately recreate the displaced bone in the orbital floor – while also building up the thickness of the orbital rim which had been displaced inferiorly. The maxilla implant restored the contours of the now deficient maxilla – meeting the new contour established on the orbital rim, while leaving clearance around the infra-orbital nerve.
