Surgical Design Case Study 5 - Hemimandibulectomy and Fibula Free Flap Reconstruction
AT: PDR
FOR: NHS
MY ROLE: RESEARCH PROJECT MANAGER / DESIGNER
PEER-REVIEWED REPORT AVAILABLE AT: Ph.D. THESIS

Clinical Background
The patient had been diagnosed with a tumour in their lower jaw (mandible). The surgeon prescribed an excision with a safe margin; and replacement of the missing portion of jaw with carefully harvested and shaped segments of the patient’s fibula bone. This ‘fibula free-flap’ was selected because it had a good blood supply – which could be re-connected at the jaw-site.
Conventionally, this procedure would have relied heavily on an individual surgical team’s (considerable) skill on a given day. A digital design and 3d-printing approach was adopted to improve the predictability of the operation; and to reduce its duration - by eliminating processes which relied on iterative bone shaping and on-the-spot judgements. Ultimately, the aim was to guarantee superior aesthetic and functional results.

Design
I worked closely with the clinical lead on this project to plan the surgical procedure digitally, and design patient-specific devices. My carefully structured design process enabled efficient implementation of clinical decisions and contingencies in this time-sensitive project. One meeting was held to specify the surgical plan, with a second used to refine and approve the final device designs.

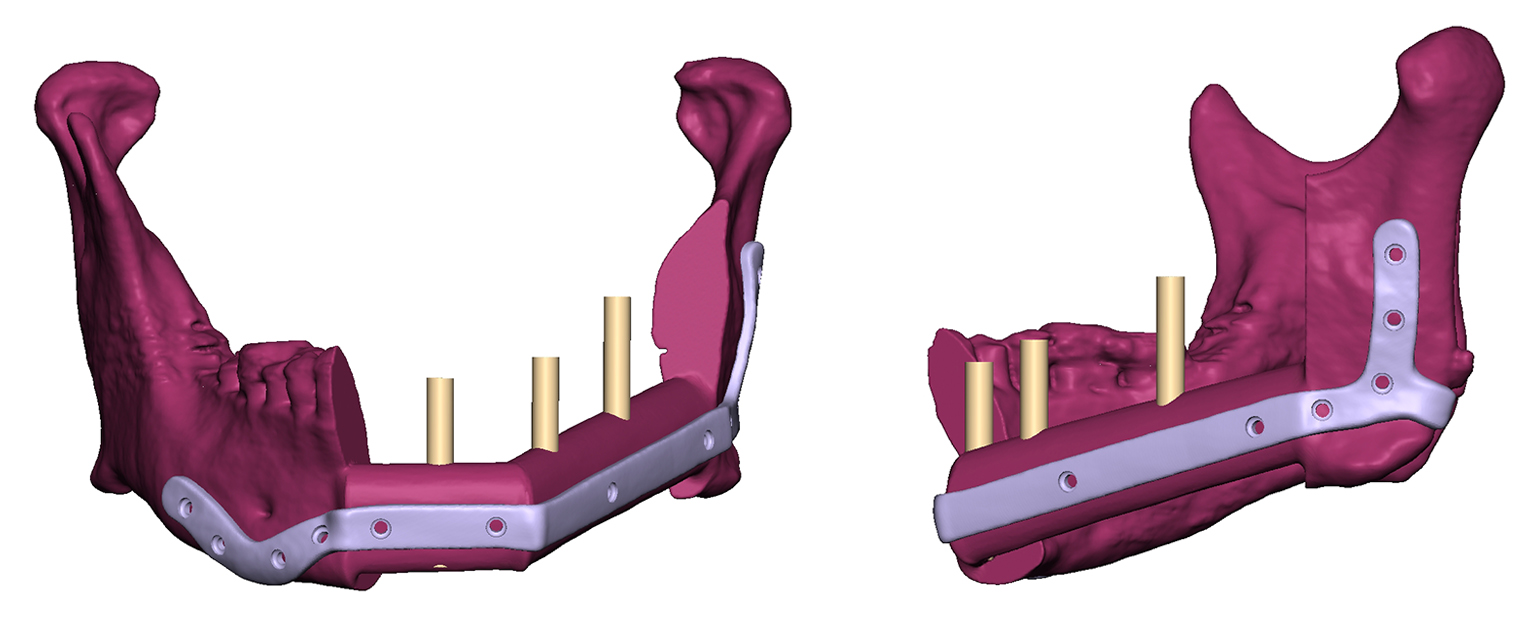
I segmented the patient’s CT scan-data and created a virtual model as the basis for digital surgical planning. The surgeon specified the cutting margins on the mandible, and the correct portions of fibula to reconstruct it. I designed patient-specific surgical guides to translate these cuts into the realities of theatre, and designed a custom implant to fit precisely against the bone segments and fix them together.
Considerations
I designed a third cutting guide to ensure that exactly the correct lengths and angles of fibula bone were harvested. The cutting guides also featured drilling holes which precisely located pilot drills – and therefore the final screw-positions for fixing the implant. Drilling “keys” – developed and supported by PDR’s research – improved the accuracy of the drill guidance, and also encouraged good irrigation.